


ORIGINAL STUDIES

Aim. To validate the European SCORE2 scale for assessing the 10-year risk of fatal and non-fatal cardiovascular events in the Russian population and to develop an adapted local version of the scale (SCORE2-RF) with defined thresholds for risk stratification.
Material and methods. The analysis was performed on data from the prospective follow-up of the Russian cohort of the ESSE-RF study (2012-2014, 10 regions). The final sample included participants aged 40-64 years without a history of cardiovascular disease (CVD) or diabetes mellitus. The median follow-up was 11.5 years. The combined endpoint included death from cardiovascular causes, non-fatal myocardial infarction, and/or stroke. Data collection involved questionnaires, anthropometry, and laboratory tests. Тo assess the associations of risk factors with the combined cardiovascular endpoint, a Fine–Gray competing risks model with stratification by region and type of settlement was used. The calculated hazard ratios were converted into absolute probabilities. The prediction accuracy of the original and adapted scales was assessed using Bland–Altman plots and calibration coefficients.
Results. The Fine–Gray model confirmed a statistically significant association with the combined endpoint for most SCORE2 components (age, systolic blood pressure, total cholesterol, smoking) in men. In women, smoking did not show a significant association (HR 1.18; 95% CI: 0.73-1.91). Validation showed that the original SCORE2 scale satisfactorily predicted risk for Russian men, slightly overestimating it (by 0.96 percentage points or by a factor of 1.11), but the prognosis for women was significantly overestimated – on average by 3.12 percentage points or by a factor of 1.72. Based on the constructed Fine–Gray model, an adapted SCORE2-RF scale was developed. To avoid shifting most of the population into the high-risk category when using the original SCORE2 thresholds, new stratification criteria were proposed, based on the percentile distribution of risk within each age-sex group (low/moderate, high, very high risk).
Conclusion. The adapted SCORE2-RF scale, developed based on Russian population data and using new threshold values, is a more accurate and practical tool for risk stratification and clinical decision-making in the Russian healthcare setting.
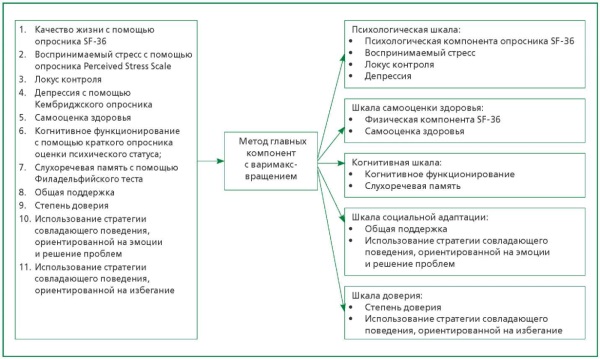
Aim. To develop new composite mental health assessment scales integrating indicators of psycho-emotional and cognitive functioning, and to analyze their associations with cardiovascular diseases (CVD) and mortality in population aged 55 and older.
Material and methods. The study was conducted as part of the prospective cohort study «Stress, Aging, and Health in Russia» (SAHR). A total of 1876 individuals (898 men and 978 women) examined between 2007-2009 were included. Using principal component analysis with varimax rotation applied to 11 initial indicators (self-rated health, quality of life, perceived stress, depression, cognitive status, auditory-verbal memory, level of trust, locus of control, general support, coping strategies), five composite scales were formed: Psychological, Self-Rated Health, Cognitive, Social Adaptation, and Trust Level. Epidemiological diagnosis of arterial hypertension, acute cerebrovascular accident (stroke), coronary artery disease (CAD), and myocardial infarction (MI) was established based on questionnaire data and instrumental examination methods. The median follow-up period was 13 years, during which 559 men and 369 women died, including 296 and 196 from CVD, respectively. Associations of the scales with CVD were analyzed using logistic regression, while associations with all-cause and CVD mortality were analyzed using Cox regression, adjusted for risk factors and CVD.
Results. In men, psychological and cognitive impairments, as well as poor self-rated health, were associated with the presence of stroke, MI, and CAD. In women, these indicators were associated only with stroke and MI (self-rated health). Regarding mortality, multivariate analysis showed that cognitive impairment and poor health according to the self-rated health scale significantly increased the risk of all-cause mortality, regardless of gender and after adjustment for socio-demographic and clinical indicators. Similar results were observed for CVD mortality. In women, problems with social adaptation were an additional risk factor for all-cause mortality
Conclusion. The developed composite mental health assessment scales were significantly associated with CVD and mortality in individuals 55 years and older. The Self-Rated Health and Cognitive Functioning scales have high predictive power for mortality risk in both genders, that highlights their importance in clinical practice for assessing overall health and prognosis.
Aim. To study the associations of rare gene variants involved in monogenic diseases presenting with low bone mineral density (BMD) and dyslipidemia, with combined vascular wall and bone tissue changes in women.
Material and methods. The study included 308 peri- and postmenopausal women aged 45 to 82 years, examined on an outpatient basis as part of cross-sectional (2018-2020) and prospective (baseline visit – 2012-2014, repeat – after 10 years) studies. Cardiovascular risk (SCORE) and fracture risk (FRAX) assessment, carotid ultrasound with atherosclerotic plaques (ASP) registration, multispiral computed tomography of the coronary arteries to assess the Agatston calcium index (ACI), measurement of BMD by dual-energy X-ray absorptiometry, molecular genetic examination using targeted sequencing were performed. Rare gene variants associated with monogenic diseases with low BMD (BMP1, COL1A1, COL1A2, ALPL, ENPP1, SLC34A1, LRP5, WNT1, FBN1, TGFBR2, LMNA, NOTCH2, PLS3) and with monogenic dyslipidemia and atherosclerosis (AS) (LDLR, APOE), were selected, which are combined and summarized according to the principle of entry into the gene’s networks (Е-ECM, Е-MIN, Е-WNT, Е-TGFB, Е-OTHER, Е-ALL, Е-ATHER).
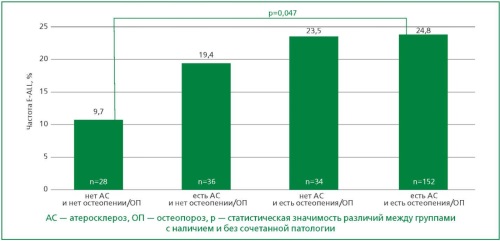
Results. Low bone mass was detected in 70.4% of women, and its combinations with signs of subclinical AS – the presence of ASP and/or ACI ≥1 unit – were noted in 60.8% of patients. Among the studied genetic factors, variants of the genes SLC34A1 (6.5%), LDLR (3.3%), COL1A2 (2.3%), LRP5 (2.3%) and the sum of variants from the groups of genes E-ALL (23.7%) and E-MIN (8.4%) were more common. In the group of women with a combination of signs of subclinical AS and osteopenic syndrome (presence of ASP and/or ACI ≥1 unit and low BMD) variants of the SLC34A1 gene (0% vs 7.2%, p=0.008) and variants from three groups of genes E-ALL (9.7% vs 24.8%, p=0.047), E-MIN (0% vs 9.2%, p=0.003), E-TGFB (0% vs 4.6%, p=0.033) were significantly more frequent compared to the group without this combination of signs. The total burden of rare variants in all genes associated with monogenic diseases with low BMD (E-ALL) increased the chance of detecting a combined pathology by 3.2 times (95%CI [1.04-9.07], p=0.047). In multivariate regression analysis (adjusted for age ≥55 years, body mass index <20 kg/m2, intima-media complex thickness ≥0.9 mm, total cholesterol ≥5.0 mmol/L, bone resorption marker CTx >1,008 ng/ml, SCORE ≥1%, FRAX ≥7% for the main fractures and FRAX ≥0.3% for hip fracture), the independent role of none of the studied genetic integral factors in the development of combined pathology has not been confirmed.
Conclusion. A clear trend towards an increased frequency of integral genetic factors, representing the sum of rare gene variants associated with monogenic diseases with low BMD was observed in patients with a combination of AS and osteopenic syndrome. This trend did not reach statistical significance, likely due to insufficient sample size or the predominance of clinical risk factors.
Aim. To study the safety of using the intravenous beta-blocker (BB) esmolol in the early stages of ST-segment elevation myocardial infarction (STEMI) before primary percutaneous coronary intervention (PCI) based on an analysis of the incidence and clinical significance of adverse events (acute heart failure, hypotension, bradycardia, disorders of atrioventricular conduction (AV conduction), etc.) compared with the control group.
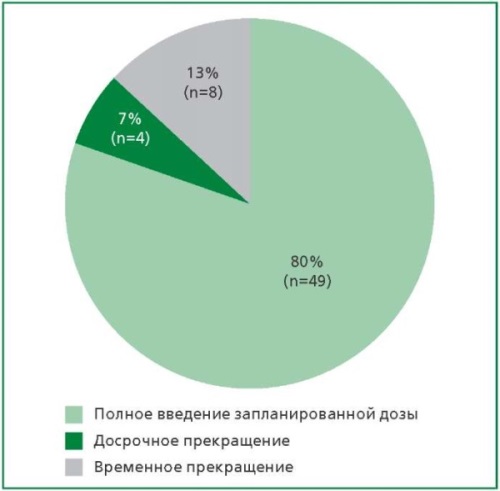
Material and methods. The presented study is part of the randomized controlled trial ESMO-VASCMI (ClinicalTrials.gov NCT number 06376630) on the study of the cardioprotective effect of IV BB esmolol in the early stages of STEMI. The study included 121 patients (n=60 in the control group and n=61 in the esmolol group) with STEMI in the first 48 hours after the onset of symptoms contraindications to BB, who were not prescribed metoprolol before PCI due to safety concerns. The administration of esmolol began with a loading dose of 500 mcg/kg for 1 minute, followed by an infusion for 6 hours. With the development of adverse events, esmolol therapy was discontinued prematurely or temporarily suspended.
Results. No statistically significant difference was observed in the frequency of adverse events potentially provoked by β1‑blocker administration between the study groups. In the esmolol group, there was a trend toward a higher incidence of bradycardia during PCI (18.03% vs 6.63%, p=0.058); hypotension (down to 70/40 mm Hg) was observed in 2 patients (3.3%), and AHF manifestations in 2 (3.3%). In 4 patients (7%), the infusion was prematurely discontinued, and in 8 (13%) it was temporarily suspended and resumed after hemodynamic stabilization. No cases of bronchospasm were detected. All cases of bradycardia and hypotension were clinically insignificant. Bradycardia developed during reperfusion with PCI, atropine was administered to 2 patients, and esmolol infusion was subsequently resumed. In the esmolol group, there was no development of stable ventricular rhythm disturbances (ventricular fibrillation (VF) or ventricular tachycardia (VT)) on the first day of the disease, in contrast to the control group (n=4; 6.67%). The differences were significant (p=0.04). The incidence of hospital deaths was low (n=1 in the control group), with no significant difference between the study and control groups (0% vs 1.7%).
Conclusion. The study results confirm the favorable safety profile of esmolol. Intravenous esmolol administration reduced the incidence of life-threatening arrhythmias without increasing the frequency of conduction disturbances, bradycardia, or AHF. In most cases, discontinuation of the infusion was sufficient to manage bradycardia in the esmolol group.
Aim. Тo conduct a preclinical trial of the effect of beetroot powder (Beta-NO-BOOST), as an exogenous source of nitrate and nitrite ions (NOx), on blood pressure (BP) and arterial stiffness in patients with arterial hypertension (AH).
Material and methods. The pilot preclinical study included 22 male volunteers (49±10 years) with AH who completed the protocol. Participants took Beta-NOBOOST beetroot powder, developed for the National Research Center for Therapeutic and Mechanics, at a dose of 20 g/day, equivalent to 650-700 mg NOx, orally for a week in addition to prescribed therapy. Blood pressure was monitored by 24-hour BP monitoring and volumetric sphygmography, which included measuring blood pressure in all four limbs and calculating the cardio-ankle vascular index (CAVI) and ankle-brachial index before and after beetroot powder intake. Blood was collected to analyze the total concentration of nitrate and nitrite ions (NOx, μM) using a colorimetric method based on the Griess reaction with single-step reduction of nitrate to nitrite using a vanadium (III) chloride solution in 1N hydrochloric acid.
Results. Serum NOx concentrations increased by an average of 2.7 times after completing the Beta-NO-BOOST beetroot powder regimen, confirming adherence to the study protocol. No significant difference in BP levels was observed before and after Beta-NO-BOOST, but a significant decrease of 0.3 units in the arterial stiffness index (CAVI) was noted. Furthermore, after a week of Beta-NO-BOOST regimen, negative correlations were found between NOx concentrations and blood pressure parameters, with a high r coefficient reaching -0.66.
Conclusion. This preclinical trial demonstrated that increased NOx concentrations in the blood were associated with decreased arterial stiffness. Based on the significant negative correlations between serum NOx levels and blood pressure, it is demonstrated that the NOx in beetroot powder contributes to lowering blood pressure. The results of the preclinical trial support the feasibility of a randomized crossover controlled clinical trial of the developed beetroot powder, Beta-NO-BOOST, as a therapeutic nutritional supplement for patients with AH.
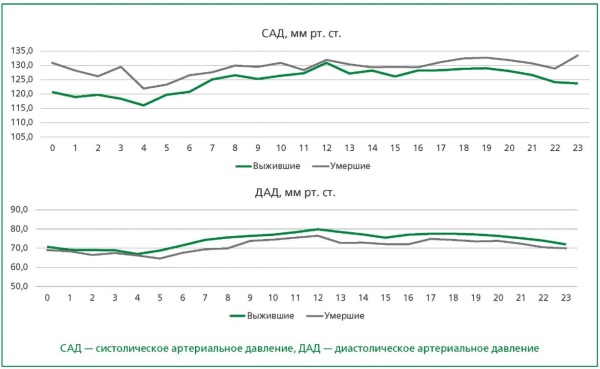
Aim. To assess the prognostic value of in-hospital 24-hour blood pressure monitoring (BPM) data in patients with arterial hypertension (AH) and other cardiovascular diseases (CVD) within the hospital registry of a multidisciplinary medical center.
Material and methods. This study was conducted as part of the REKVAZA-CLINICA NMIC TPM hospital registry. The final analysis included 358 patients with a mean age at hospitalization of 72.9±12.0 years (median 74.0 [28.7; 97.6] years). Over a mean prospective follow-up period of 9.4±2.3 years (median 10.2 [0.4; 11.5] years), the primary endpoint (PE; all-cause mortality) was recorded in 77 (21.5%) patients. The secondary composite endpoint (SCE) — composing non-fatal acute myocardial infarction and/or non-fatal acute cerebrovascular accident and/or pulmonary embolism and/or relevant surgical interventions and/or hospitalization for concomitant CVD — was identified in 160 (44.7%) patients.
Results. Multivariate analysis in the patient group aged <75 years (n=197) showed that the risk of PE was associated with the presence of concomitant CVD (HR=3.25; 95% CI=1.14-9.22; p=0.027), higher average real variability of systolic BP (HR=1.19; 95% CI=1.01-1.41; p=0.038), and higher mean 24-h pulse pressure (PP) (HR=1.05; 95% CI=1.02-1.09; p=0.001). In the group of patients aged ≥75 years (n=161), PE was associated only with age (HR=1.17; 95% CI=1.12-1.23; p<0.001). In the overall patient cohort (n=358), PE was associated with the riser BP pattern (HR=3.93; 95% CI=1.44-10.73; p=0.008). The SCE was associated with the presence of concomitant CVD (HR=1.88; 95% CI=1.35-2.62; p<0.001) and higher mean daytime PP (HR=1.14; 95% CI=1.08-1.20; p<0.001).
Conclusion. In patients with AH, 24-h BPM parameters obtained in a hospital setting retain their prognostic value, despite the significant impact of cardiovascular comorbidity and age on outcomes.
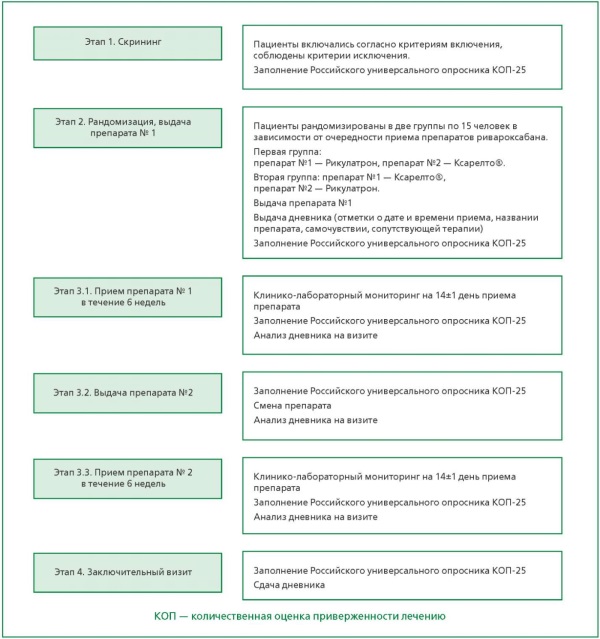
Aim. To study the therapeutic equivalence (efficacy, safety, and tolerability) and pharmacokinetics of the brand-name and generic rivaroxaban 20 mg in patients with non-valvular atrial fibrillation and a high risk of thromboembolic complications.
Material and methods. This open-label, randomized, crossover comparative study of two 20 mg rivaroxaban tablet formulations registered in Russia, Riqulatron (Gedeon Richter OJSC, Hungary) and Xarelto® (Bayer Pharma AG, Germany), included 30 patients (16 men), with a median age of 66 years and a СHA2DS2-VASc score of 3.0 (2.3-4.0). The clinical part consisted of: a screening period (1-7 days before randomization), two 42-day rivaroxaban treatment periods with a visit on day 14±1 of each, an interim visit for drug switching, and a final visit. Patients completed a drug intake diary and an adherence questionnaire. Quantitative determination of rivaroxaban concentration in patient plasma was performed using high-performance liquid chromatography with tandem mass spectrometric detection (HPLC-MS/MS). Data were processed using StatSoft Statistica 13.0 (USA).
Results. Data are presented for 29 patients. The steady-state trough and peak concentrations were 22.29 (3.78-101.76) ng/ml and 197.04 (118.00-376.78) ng/ml for the generic, and 20.55 (5.02-82.29) ng/ml and 179.38 (102.80-335.71) ng/ml for the brand-name drug, respectively. The 90% confidence intervals for the ratios of trough and peak concentrations were 0.93-1.25 and 0.99-1.21, respectively. Mean laboratory values for patients, regardless of the treatment sequence, were within reference ranges except for peak prothrombin time. Rivaroxaban concentration was a significant predictor of prothrombin time (p<0.001), with a strong direct correlation between these parameters. No thromboembolic events were recorded in any patient during the observation period. Hemorrhagic complications (gingival bleeding, hematuria) were recorded in ten patients; five events occurred while taking the brand-name drug and seven while taking the generic; no rivaroxaban discontinuation was required. Other adverse events (laboratory value deviations from reference ranges, decompensation of chronic heart failure, paroxysm of atrial fibrillation, diarrhea) also did not require rivaroxaban discontinuation.
Conclusion. The comparative study of the two rivaroxaban formulations demonstrated similar efficacy, safety, tolerability, and pharmacokinetics for Riqulatron (Gedeon Richter OJSC, Hungary) and Xarelto® (Bayer Pharma AG, Germany) at a 20 mg dose in patients with non-valvular atrial fibrillation.
Aim. To define the proportion of comorbid chronic kidney disease (CKD) in the cohort of patients with coronary artery disease (CAD) and to estimate the incidence of comorbidities and required cardiovascular pharmacotherapy on a basis of united data from several medical registries.
Material and methods. We have analyzed the united data from 11 registries of patients with cardiovascular diseases (CVD) created in 6 regions of Russia under the supervision of the National Medical Research Center for Therapy and Preventive Medicine. There are 13089 patients with IHD in those registries including 1419 (10.8%) with CAD and CKD combination (36.6% men, age 73.1±9.4 years), 10649 (81.4%) patients with CAD without CKD (48.9% men, age 68.2±9.4 years). There are 1021 (7.8%) patients without convincing data for presence or absence of CKD. The CAD criterion was registration of this diagnosis in medical documents. The CKD criterion was registration of this diagnosis in medical documents and/or low glomerular filtration rate (<60 ml/min/1.73 m2) revealed at least twice with an interval not less than 3 months.
Results. The incidence of cardiovascular multimorbidity in patients with CAD and CKD combination was bigger than in patients with CAD without CKD (96.0% vs 90.3%; р<0.001). The average number of CVD (2.85±0.8 vs 2.54±0.83; p<0.01) was also bigger, including the subgroups with history of myocardial infarction (MI (2.96±0.8 vs 2.6±0.86; р<0.01)) and acute cerebrovascular accident (ACVA (2.96±0.8 и 2.6±0.86; р<0.01)), with diabetes (2.95±0.75 vs 2.66±0.8; р<0.01). It was no significant difference of the incidence of required cardiovascular pharmacotherapy in cases of CAD with and without CKD (58.4% vs 57.6%; р=0.15). This value in patients with CAD and CKD combination was bigger if to compare cases of presence and absence of history of MI (65.4% vs 52.7%; р<0.0001), of ACVA (60.1% vs 57.5%; р<0.0001), but was lower in cases with diabetes mellitus (55.9%) than without diabetes mellitus (59.9%); р=0.0005.
Conclusion. The pooled data of 11 registries of patients with CAD demonstrated 10.8% rate of the combination with CKD. The incidence of cardiovascular multimorbidity, average number of CVD in patients with CAD and CKD combination were significantly bigger in cases of diabetes and history of MI and ACVA. The incidence of required cardiovascular pharmacotherapy accordingly the main indications in patients with CAD and CKD combination was insufficient (58%) and was some bigger in subgroups with history of MI and ACVA but lower in presence of diabetes (55.9%). In patients with CAD and CKD combination, especially against the background of diabetes mellitus, it is necessary to increase the frequency of prognostically significant cardiovascular pharmacotherapy in clinical practice.
PAGES OF RUSSIAN NATIONAL SOCIETY OF EVIDENCE-BASED PHARMACOTHERAPY
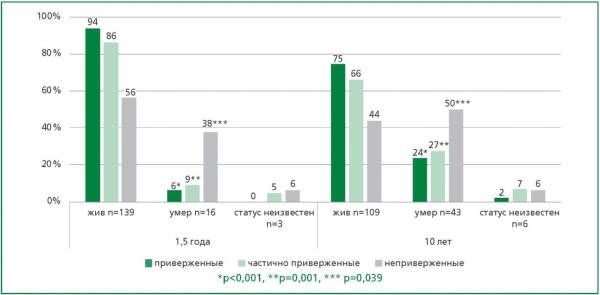
Aim. To assess the impact of treatment adherence on long-term outcomes over a ten-year period in patients with acute myocardial infarction (MI) based on data from the prospective PROFILE-MI registry.
Material and methods. The prospective PROFILE-IM registry included 160 patients attended a cardiologist at Moscow City Polyclinic No. 9 or one of its two branches in the period from March 1, 2014 to December 31, 2015. The vital status of patients was assessed 10 years after their discharge from the hospital.
Results. Analysis of the results of the NODF Adherence Scale survey made it possible to identify three categories of patients (n=158, two patients refused to fill out the questionnaire): committed – 98 (62%), non-committed – 16 (10%), partially committed – 44 (28%). The life status was analyzed after 1.5 and 10 years in patients of these groups, with a 95% response rate. At 1.5 years from the start of observation, fatal outcomes were recorded in 16 (10%) patients. After ten years of follow-up, the number of deaths increased to 43 (26.9%) patients. Patients who developed primary endpoint (PEP) were significantly older than those without it – 70.3±11.1 vs 58.6±10.5 years, p<0.001. According to multivariate analysis, the risk PEP developing during a ten-year follow-up was 2.7 times higher in non-adherent patients compared to adherent and partially adherent patients (p=0.027). The ten-year monitoring data indicate that the probability of PEP increases by 8.6% every year of the patient’s life.
Conclusion. The results of the study demonstrate that insufficient treatment adherence increases the likelihood of an adverse outcome during the ten-year followup period. Long-term monitoring of patients with insufficient treatment adherence is of particular importance in the context of secondary prevention.
CLINICAL CASE
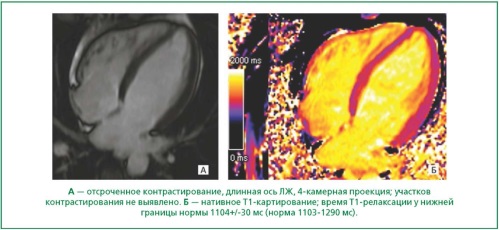
The article presents a clinical case of familial PRKAG2-cardiomyopathy, illustrating diagnostic challenges and the importance of molecular genetic verification. A comprehensive clinical and instrumental examination of the proband and close relatives was performed, along with whole-exome sequencing. The proband, with a family history of sudden cardiac death, was found to have apical hypertrophy of the left ventricle, a history of supraventricular extrasystole, and atrial fibrillation. Her younger son was documented to have ventricular pre-excitation syndrome, bradycardia, and syncopal episodes. Genetic analysis identified a heterozygous pathogenic variant c.905G>A (p.Arg302Gln; rs121908987) in the PRKAG2 gene in both the proband and her younger son. The described case emphasizes that cardiomyopathy associated with the p.Arg302Gln variant can present with moderate myocardial hypertrophy, while electrophysiological disturbances (pre-excitation, bradyarrhythmias) and a burdened family history of sudden death take precedence in the clinical picture. Thus, the combination of conduction disorders (especially WPW syndrome) with mild hypertrophy and familial cases of sudden death forms a characteristic «red flag» for this disease. The presence of such a combination of signs in the family history necessitates targeted genetic testing for diagnosis verification and correct risk stratification.
CURRENT QUESTIONS OF CLINICAL PHARMACOLOGY
Aim. To analyse the frequencies of the CYP2C19 gene alleles and genotypes associated with the metabolism of antiplatelet agents in patients with coronary artery disease (CAD), considering potential drug-drug interactions in real clinical practice in Arkhangelsk.
Material and methods. The cross-sectional study was conducted at the Emergency Cardiology Department of the Regional Vascular Center of the E.E. Volosevich First City Clinical Hospital in Arkhangelsk. The study included 96 patients diagnosed with CAD (I20.0-I22.0 according to ICD-10). Patients were divided into two groups: those hospitalized for the first time and those readmitted. All patients underwent pharmacogenetic testing of polymorphic variants of the CYP2C19 gene. Genotyping of polymorphic variants of the CYP2C19 gene was performed using the polymerase chain reaction (PCR) method in real time. The analysis of allelic variants rs28399504, rs4244285, rs4986893 of the CYP2C19 gene was performed on a Bio-Rad CFX96 Touch amplifier using the SNP-Screen kits (Synthol LLC, RF).
Results. The study included 96 patients with CAD aged 39 to 100 years. The patients were divided into two groups: primarily hospitalised and patients readmitted for recurrent acute coronary syndrome. The groups were comparable in sex and age. Significant differences were observed for INR: 1.05 [1.00; 1.14] in the first group and 1.08 [1.03; 1.14] in the second group (p=0.04), as well as for treatment outcome – 4 fatal cases (10%) were noted in the second group, while all patients in the first group were discharged (p=0.016). In both groups, carriers of low-functional CYP2C19 variants (G681A, G636A), classified as intermediate or poor metabolisers, were identified in both groups, which may be significant for drug-drug interactions in CAD pharmacotherapy in clinical practice. The A1G variant was identified only in the first group (3,6% (n=2)). No statistically significant difference was found in the frequency of loss-of-function alleles between the groups or in the
frequency of readmissions during antiplatelet therapy. Analysis of therapy in patients carrying pathological alleles revealed potentially adverse drug-drug interactions, e.g., clopidogrel and omeprazole, manifested as reduced clopidogrel efficacy and an increased risk of gastrointestinal bleeding.
Conclusion. This study did not reveal a statistically significant association between the presence of mutant CYP2C19 gene alleles and the frequency of readmissions, but emphasized the importance of a comprehensive personalized approach to pharmacotherapy in CAD patients. Consideration of pharmacogenetic, clinical, and pharmacological factors may contribute to therapy optimization and improvement of CAD treatment outcomes. Further studies with larger samples (including population-based studies) are required for definitive conclusions.

ISSN 2225-3653 (Online)






































.jpg)

